
Download
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) Research Data (1973-2014), National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2018, based on the November 2017 submission
Article
Increased utilization of external beam radiotherapy relative to cystectomy for localized, muscle-invasive bladder cancer: a SEER analysis
Tyler J. Wilhite1, David Routman1, Andrea L. Arnett1, Amy E. Glasgow2, Elizabeth B. Habermann2, Thomas M. Pisansky1, Stephen A. Boorjian3, Krishan R. Jethwa1, Lance A. Mynderse3, Kristofer W. Roberts1, Igor Frank3, Richard Choo1, Brian J. Davis1, Bradley J. Stish1
1Department of Radiation Oncology, Mayo Clinic, Rochester, MN, USA
2Robert and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN, USA
3Department of Urology, Mayo Clinic, Rochester, MN, USA
2Robert and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN, USA
3Department of Urology, Mayo Clinic, Rochester, MN, USA
Corresponding author: Bradley J. Stish, Email: stish.bradley@mayo.edu
Competing interests: The authors have declared that no competing interests exist.
Abbreviations used: ACM, all-cause mortality; CSM, cause-specific mortality; CSS, cause-specific survival; MIBC, muscle-invasive bladder cancer; OS, overall survival; RT, radiotherapy; SEER, surveillance, epidemiology, and end results program
Received November 21, 2017; Revision received April 10, 2018; Accepted June 13, 2018; Published August 23, 2018
Abstract
Objective: To assess recent utilization patterns of radiotherapy (RT) relative to cystectomy for muscle-invasive bladder cancer (MIBC) and evaluate survival trends over time in patients receiving RT.
Materials and Methods: The surveillance, epidemiology, and end results program (SEER) was used to identify patients diagnosed between 1992 and 2013 with localized MIBC. Patients with a prior history of non-bladder malignancy, who received no treatment, or did not have available treatment information, were excluded. Treatment utilization patterns were assessed using Cochran-Armitage tests for trend, and patient characteristics were compared using chi-square tests. Overall survival (OS) and cause-specific survival (CSS) were estimated using the Kaplan-Meier method. All-cause (ACM) and cause-specific mortality (CSM) were evaluated with multivariable Cox proportional hazards regression.
Results: Of 16175 patients analyzed, 11917 (74%) underwent cystectomy, and 4258 (26%) were treated with RT. Patients who received RT were older (median age 79 vs. 68, P < 0.01). Over time, the proportion of patients receiving RT relative to cystectomy increased (24% 1992–2002 vs. 28% 2003–2013, P < 0.01), despite median patient age throughout the study period remaining unchanged (71 for each 1992–2002 and 2003–2013, P = 0.41). For RT, compared with patients diagnosed earlier, those diagnosed from 2010–2013 showed improved OS (64% vs. 60% at 1 year, P < 0.01; 38% vs. 29% at 3 years, P < 0.01) and CSS (71% vs. 67% at 1 year, P = 0.01; 51% vs. 40% at 3 years, P < 0.01). On multivariable analysis, diagnosis from 2010–2013 was associated with a lower estimated risk of ACM (hazard ratio 0.77; 95% confidence interval 0.66–0.89, P < 0.001) and CSM (hazard ratio 0.81; 95% confidence interval 0.67–0.97, P = 0.02).
Conclusion: Utilization of RT for localized MIBC increased relative to cystectomy from 1992 to 2013, despite the median age of treated patients remaining unchanged. More recent survival outcomes for patients receiving RT were improved, supporting continued use of bladder preservation strategies utilizing RT.
Keywords: bladder cancer, SEER, radiotherapy, cystectomy
Introduction
Bladder cancer will afflict an estimated 80000 patients in 2017 and result in 17000 deaths [1]. While most patients present with superficial tumors that are highly treatable, 30% have muscle-invasive disease that carries a higher risk of progression and mortality [2]. For patients with muscle-invasive bladder cancer (MIBC), radical cystectomy is the most commonly used definitive treatment, and large surgical series report 5-year overall survival (OS) rates nearing 60% [3-6]. However, for appropriately selected patients, bladder preservation therapy consisting of maximal transurethral resection of bladder tumor followed by external beam radiotherapy (RT) typically with concurrent chemotherapy stands as a reasonable alternative [7,8].
Multiple prospective trials have demonstrated bladder preservation therapy to be feasible, with favorable results that are comparable to those obtained with cystectomy [8-12]. Nonetheless, prior population-based studies showed that RT for bladder preservation is infrequently utilized as compared with surgery. A Surveillance, Epidemiology, and End Results program (SEER) analysis of patients with localized MIBC diagnosed from 1988 to 2006 showed that 86% of patients had surgery, 11% received RT, and that utilization rates of RT did not increase over that timeframe [13]. A notable limitation of that study was that RT was compared to a broad, poorly defined category of surgery that included procedures ranging from radical cystectomy to non-definitive local treatments, such as transurethral resection. We aimed to perform an updated SEER analysis to determine whether the utilization rate of RT for bladder preservation therapy in direct comparison to surgery had changed more recently. Furthermore, we sought to evaluate trends in recent survival outcomes for patients receiving RT.
Materials and Methods
Study population and study design
We used the SEER database to identify 275843 patients diagnosed from 1992 to 2013 with localized MIBC (stages II-III; topography codes C67.0-C67.9) and urothelial carcinoma, squamous cell carcinoma, or adenocarcinoma histology [14]. Patients with noninvasive or T1 disease were not included. The SEER program is sponsored by the National Cancer Institute and is comprised of 18 cancer registries. Its database includes population-based cancer incidence, treatment, and survival data covering approximately 28% of the United States population. We selected 1992 as the first year of this study since it is when a number of new registries joined the program, and it allowed for analysis of a sufficient duration of time to assess trends. Patients were eligible for inclusion if they received either RT or cystectomy as initial definitive treatment. Cystectomy was defined as radical or partial. Patients were excluded who had a prior history of non-bladder malignancy or who were younger than age 18 at time of diagnosis. Patients who had initial treatment other than cystectomy or RT, had no treatment, or for whom treatment information was not available were also excluded, leaving 16175 patients for the primary analysis.
Statistical analyses
Patient and tumor characteristics were compared using chi-square tests and Student’s t-test. Treatment utilization patterns over time were assessed using Cochran-Armitage tests for trend. OS and cause-specific survival (CSS) were estimated using the Kaplan-Meier method. All-cause (ACM) and cause-specific mortality (CSM) were evaluated using multivariable Cox proportional hazards regression, adjusting for age, sex, race, marital status, tumor grade, histology, year of diagnosis, and stage. All P values reported were two-sided, with those ≤ 0.05 deemed statistically significant. Statistical analyses were performed using SAS statistical software (SAS version 9.4; SAS Institute Inc., Carey, NC). As this study used de-identified SEER data, it did not require Institutional Review Board approval.
Results
Patient characteristics
Patient and tumor characteristics are shown in Table 1. The total study population consisted of 16175 patients, of whom 11917 (73.6%) received cystectomy and 4258 (26.3%) received RT. Statistically significant differences between these two groups were noted with regard to age, sex, race, marital status, tumor grade, histology, and stage (P < 0.0001 for each variable). Patients who received RT were older (median age 79 vs. 68, P < 0.01), and the only age group of patients in which the majority received RT was those 80 years or older. Other variables associated with a higher likelihood of receipt of RT were black race, widowed or unmarried marital status, and increasing tumor grade. Patients of all stages were more likely to receive cystectomy than RT, but of patients who received RT, the majority had T2 disease (76.2%, compared to 50.1% in patients who had cystectomy). T4 disease was present in relatively few patients included for analysis (5.9% of total).
Utilization of RT over time
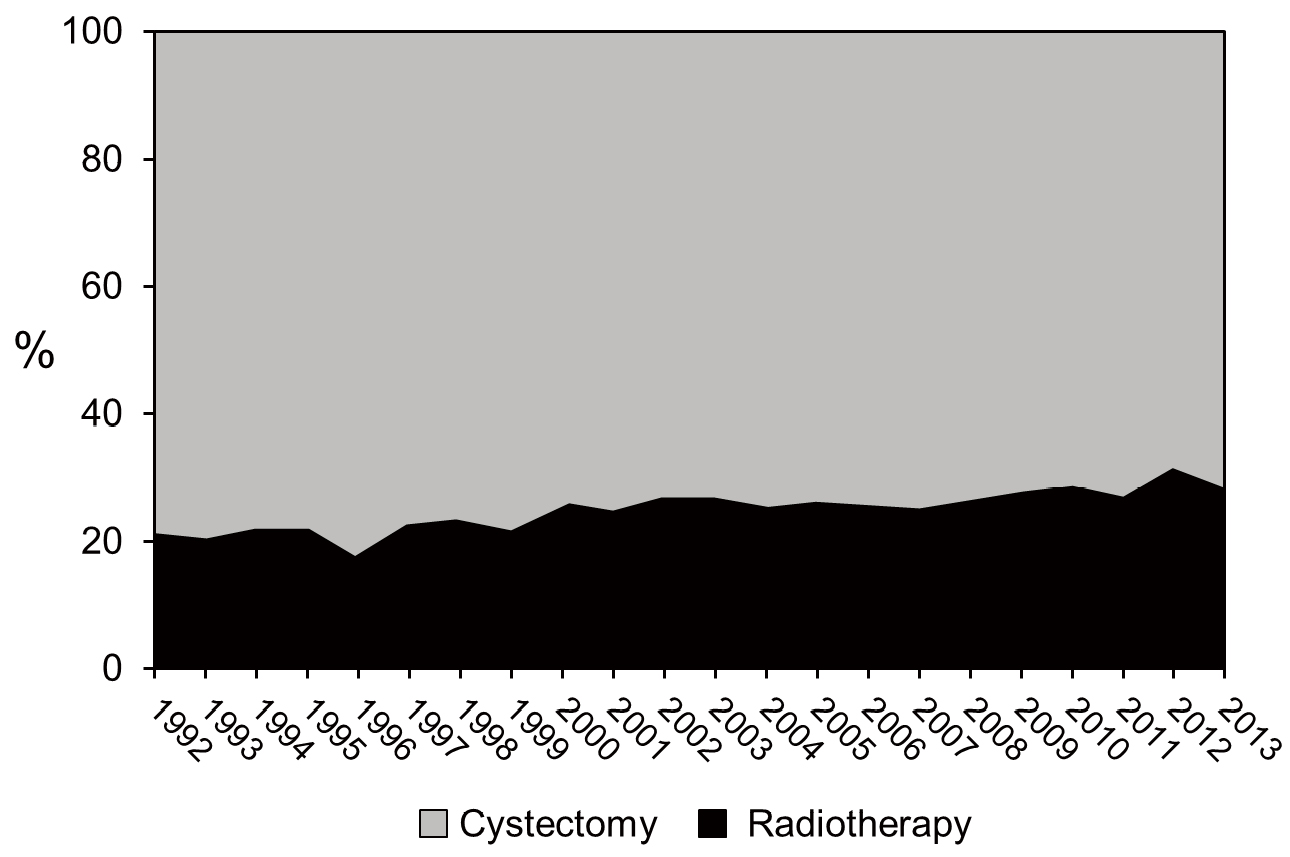
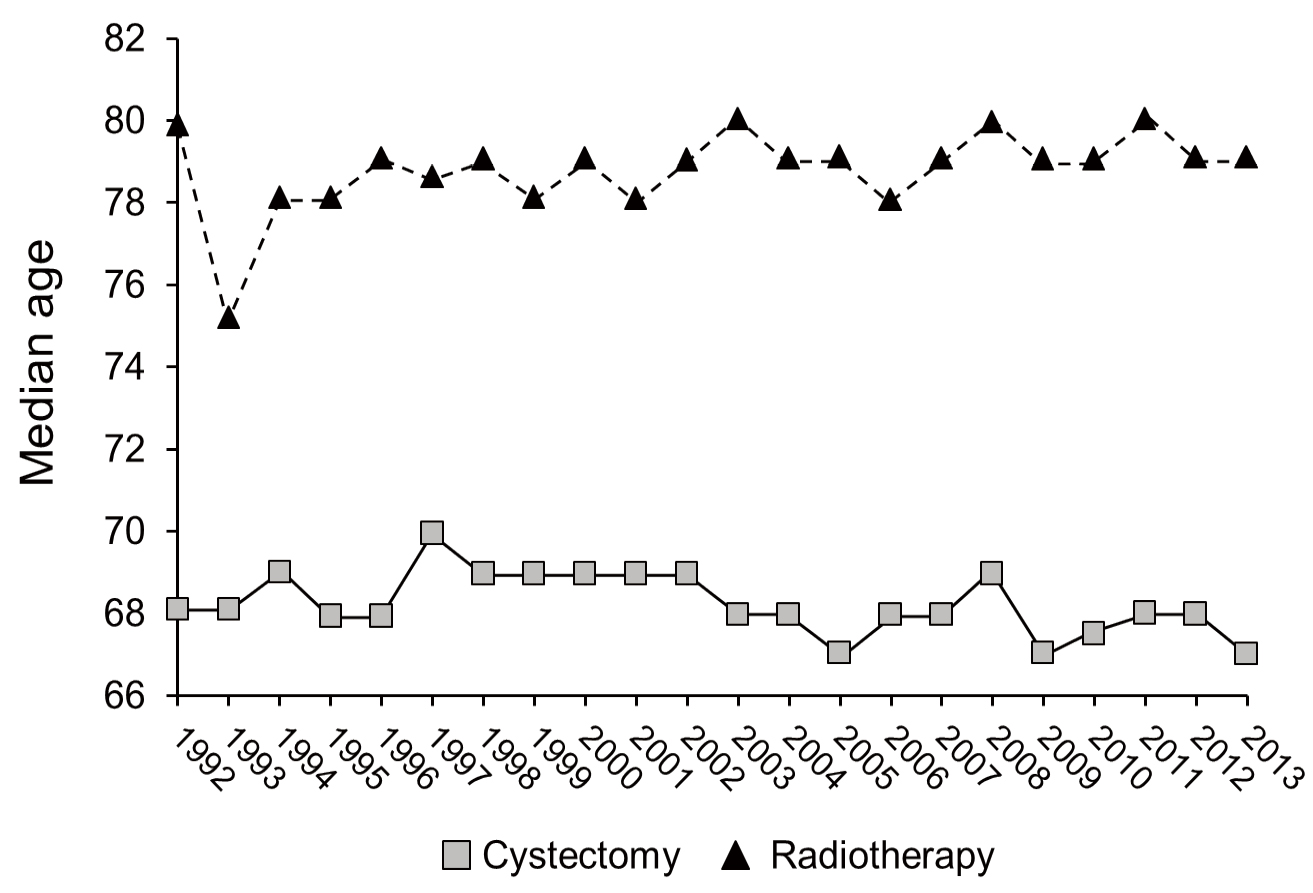
Figure 1 shows the percent utilization of RT for localized MIBC over time compared with cystectomy. While cystectomy was utilized more frequently than RT throughout the study period, there was a statistically significant increase in the proportion of patients receiving RT (24% in 1992–2002 vs. 28% in 2003–2013, P < 0.01) over time. This increase occurred in the context of no change in median patient age (71 for each 1992–2002 and 2003–2013, P = 0.41). The median patient age by treatment group over the study period is shown in Figure 2. Over the study period, the number of patients treated with either modality increased from 1.66 per 100000 person-years in 1992 to 3.24 per 100000 person-years in 2013; the yearly average for the cohort (1992–2013) was 2.70 per 100000 person-years.
Overall and cause-specific survival with RT
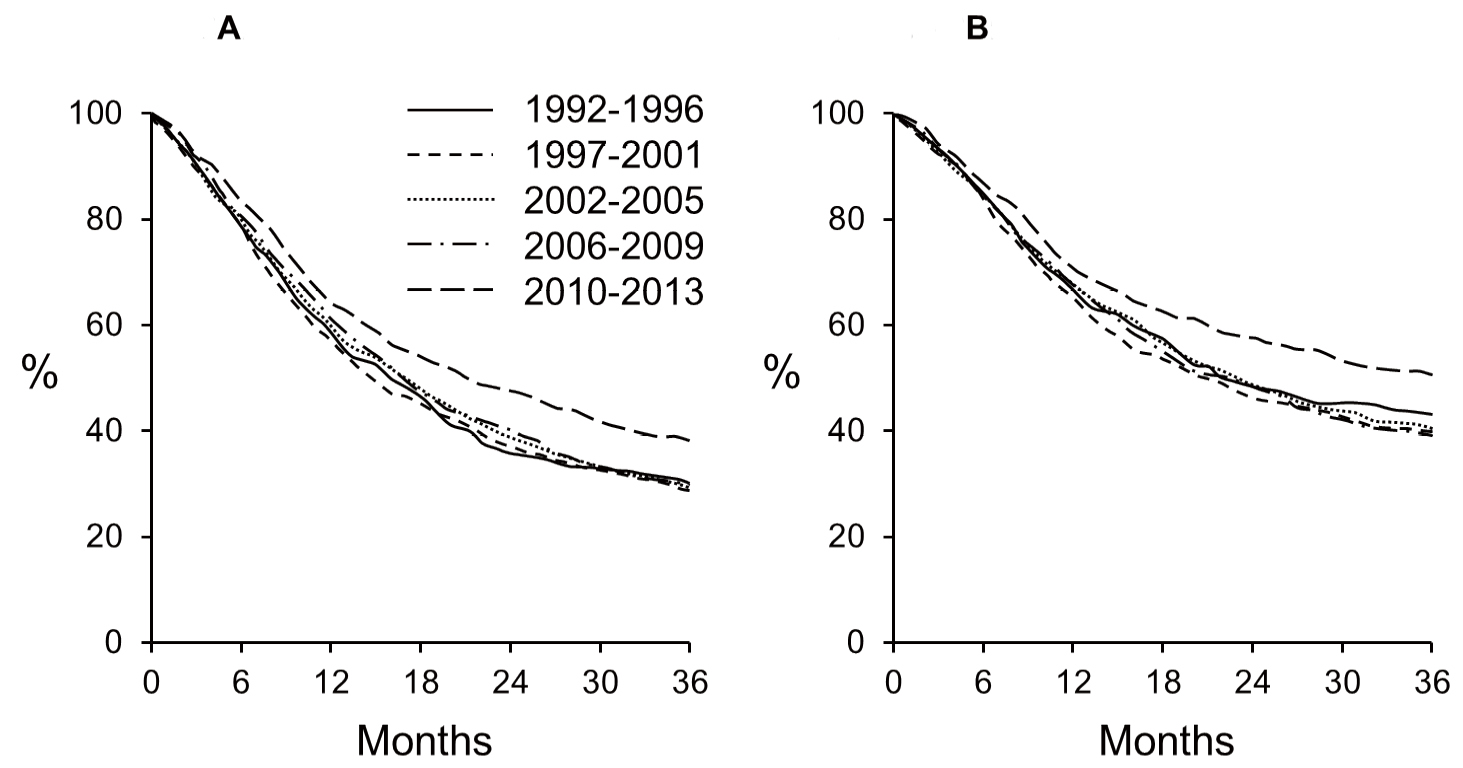
Figure 3 shows 3-year OS (Fig. 3A) and CSS (Fig. 3B) for patients receiving RT, and not cystectomy, for localized MIBC. Patients are stratified into five groups based on year of diagnosis to highlight observed differences in outcome over time. Compared with patients diagnosed from 1992 to 2009, those diagnosed from 2010 to 2013 had improved OS (64% vs. 60% at 1 year, P < 0.01; 38% vs. 29% at 3 years, P < 0.01) and CSS (71% vs. 67% at 1 year, P = 0.01; 51% vs. 40% at 3 years, P < 0.01).
Multivariable analyses of ACM and CSM are shown in Table 2 and Table 3, respectively. Increasing age, as compared with the reference group of 21–49 years old, was associated with an increased risk for both ACM and CSM. While there was no observed difference in ACM with regard to sex, CSM was less in men relative to women (adjusted HR 0.86, P < 0.01). With regard to race, outcomes in black patients and relative white patients were significantly worse for both ACM (adjusted HR 1.22, P < 0.01) and CSM (adjusted HR 1.31, P < 0.01). Similarly, as compared with patients who were married, outcomes were worse for patients who were single (adjusted HR for ACM 1.24, P < 0.01; adjusted HR for CSM 1.18, P < 0.05) or divorced (adjusted HR for ACM 1.35, P < 0.001; adjusted HR for CSM 1.35, P < 0.001).
While there was no observed association between tumor grade and survival, there were higher estimates of mortality for squamous cell histology as compared with urothelial carcinoma (adjusted HR for ACM 1.38, P < 0.001; adjusted HR for CSM 1.34, P < 0.01). Relative to urothelial histology, the proportion of non-urothelial cancers decreased from 11.4% in 1992 to 6.0% in 2013 (P < 0.001), with a gradual decline over the study period. Another tumor feature significantly associated with adverse outcomes was T4 disease (adjusted HR for ACM 1.38, P < 0.001; adjusted HR for CSM 1.57, P < 0.001). When assessing year of diagnosis in multivariable analysis, those diagnosed from 2010 to 2013 had lower estimates of mortality as compared with the reference group of 1992 to 1996 (adjusted HR for ACM 0.77, P < 0.001; adjusted HR for CSM 0.81, P = 0.02). For all other years of diagnosis evaluated (1997 to 2001, 2002 to 2005, and 2006 to 2009), ACM and CSM did not differ significantly from the reference range.
Table 1. Patient and tumor characteristics by treatment received.
| Characteristic | No. of patients (%) | Radiotherapy (%) | Cystectomy (%) | P value* | |
|---|---|---|---|---|---|
| Total | 16175 (100) | 4258 (26.3) | 11917 (73.6) | < 0.0001 | |
| Age (years) | < 0.0001 | ||||
| 21–50 | 836 (5.2) | 67 (8.0) | 769 (92.0) | ||
| 50–59 | 2311 (14.3) | 253 (10.9) | 2058 (89.1) | ||
| 60–69 | 4346 (26.9) | 645 (14.8) | 3701 (85.2) | ||
| 70–79 | 5130 (31.7) | 1292 (25.2) | 3838 (74.8) | ||
| 80–89 | 3191 (20.3) | 1726 (54.1) | 1465 (45.9) | ||
| ≥ 90 | 361 (2.2) | 275 (76.2) | 86 (23.8) | ||
| Sex | < 0.0001 | ||||
| Male | 11781 (72.8) | 2974 (25.2) | 8807 (74.8) | ||
| Female | 4394 (27.2) | 1284 (29.2) | 3110 (70.8) | ||
| Race | < 0.0001 | ||||
| White | 13488 (83.4) | 3524 (26.1) | 9964 (73.9) | ||
| Hispanic | 860 (5.3) | 192 (22.3) | 668 (77.7) | ||
| Black | 1046 (6.5) | 357 (34.1) | 689 (65.9) | ||
| Asian or Pacific Islander | 701 (4.3) | 168 (24.0) | 533 (76.0) | ||
| Other or unknown | 80 (0.4) | 17 (21.2) | 63 (78.8) | ||
| Marital status | < 0.0001 | ||||
| Single | 1680 (10.4) | 413 (24.6) | 1267 (75.4) | ||
| Married | 9802 (60.6) | 2185 (22.3) | 7617 (77.7) | ||
| Separated | 146 (0.9) | 27 (18.5) | 119 (81.5) | ||
| Divorced | 1387 (8.6) | 324 (23.4) | 1063 (76.6) | ||
| Widowed | 2664 (16.5) | 1167 (43.8) | 1497 56.2) | ||
| Unmarried or domestic partner | 8 (0.05) | 3 (37.5) | 5 (62.5) | ||
| Unknown | 488 (3.0) | 139 (28.5) | 349 (71.5) | ||
| Tumor differentiation | < 0.0001 | ||||
| Well | 157 (1.0) | 29 (18.5) | 128 (81.5) | ||
| Moderately | 1165 (7.2) | 237 (20.3) | 928 (79.7) | ||
| Poorly | 6828 (42.2) | 1796 (26.3) | 5032 (73.7) | ||
| Undifferentiated | 7442 (46.0) | 1988 (26.7) | 5454 (73.3) | ||
| Histology | < 0.0001 | ||||
| Urothelial cell carcinoma | 14895 (92.1) | 4038 (27.1) | 10857 (72.9) | ||
| Squamous cell carcinoma | 779 (4.8) | 169 (21.7) | 610 (78.3) | ||
| Adenocarcinoma | 501 (3.1) | 51 (10.2) | 450 (89.8) | ||
| Stage | < 0.0001 | ||||
| T2 | 9219 (57.0) | 3245 (35.2) | 5974 (64.8) | ||
| T3 | 6000 (37.1) | 784 (13.1) | 5216 (86.9) | ||
| T4 | 956 (5.9) | 229 (24.0) | 727 (76.0) | ||
*Chi square value pertaining to treatment and variable of interest.
Table 2. Multivariable Cox model of all-cause mortality for patients receiving RT for bladder cancer.
| Variable | HR (95% CI) | P value | |
|---|---|---|---|
| Age (years) | |||
| 21–49 | 1.00 (ref) | ||
| 50–59 | 1.21 (0.84–1.74) | 0.309 | |
| 60–69 | 1.55 (1.10–2.20) | 0.013 | |
| 70–79 | 2.31 (1.65–3.25) | < 0.001 | |
| 80–89 | 2.86 (2.04–4.01) | < 0.001 | |
| ≥ 90 | 3.96 (2.7565.69) | < 0.001 | |
| Sex | |||
| Female | 1.00 (ref) | ||
| Male | 0.98 (0.90–1.07) | 0.627 | |
| Race | |||
| White | 1.00 (ref) | ||
| Hispanic | 0.94 (0.78–1.13) | 0.527 | |
| Black | 1.22 (1.06–1.39) | 0.004 | |
| Asian | 0.84 (0.69–1.02) | 0.077 | |
| Other or unknown | 0.92 (0.47–1.77) | 0.791 | |
| Marital status | |||
| Married | 1.00 (ref) | ||
| Single | 1.24 (1.09–1.42) | 0.002 | |
| Separated | 1.26 (0.82–1.94) | 0.302 | |
| Divorced | 1.35 (1.16–1.57) | < 0.001 | |
| Widowed | 1.04 (0.94–1.14) | 0.448 | |
| Unmarried | 1.07 (0.15–7.64) | 0.947 | |
| Unknown | 1.15 (0.93–1.43) | 0.187 | |
| Tumor differentiation | |||
| Well | 1.00 (ref) | ||
| Moderately | 1.30 (0.83–2.06) | 0.255 | |
| Poorly | 1.23 (0.79–1.90) | 0.357 | |
| Undifferentiated | 1.20 (0.77–1.85) | 0.419 | |
| Unknown | 1.39 (0.87–2.20) | 0.165 | |
| Histology | |||
| Urothelial carcinoma | 1.00 (ref) | ||
| Adenocarcinoma | 0.85 (0.59–1.23) | 0.395 | |
| Squamous cell carcinoma | 1.38 (1.15–1.65) | < 0.001 | |
| Year of diagnosis | |||
| 1992 to 1996 | 1.00 (ref) | ||
| 1997 to 2001 | 1.01 (0.88–1.15) | 0.936 | |
| 2002 to 2005 | 0.98 (0.86–1.12) | 0.777 | |
| 2006 to 2009 | 0.92 (0.80–1.05) | 0.207 | |
| 2010 to 2013 | 0.77 (0.66–0.89) | < 0.001 | |
| Stage | |||
| T2 | 1.00 (ref) | ||
| T3 | 1.08 (0.98-1.19) | 0.132 | |
| T4 | 1.38 (1.17-1.62) | <0.001 | |
Discussion
Despite longstanding efforts to establish bladder preservation utilizing RT as an alternative to cystectomy for the initial management of muscle-invasive bladder cancer, adoption of this approach has primarily been limited to patients who are deemed medically inoperable. Our data from a large national registry are the first to show that utilization of RT for localized MIBC has increased relative to cystectomy. This trend occurred with no associated change in median patient age throughout the study period of 1992 to 2013, which mitigates the potential confounding effect of age on this comparison. Our analysis is the most recent to evaluate trends of RT for bladder preservation in the United States and is the first to compare these directly with rates of definitive surgery (i.e., cystectomy or partial cystectomy). While the observed absolute magnitude of increase was modest (4% over the study period), it suggests a positive trend that may reflect clinical incorporation of the growing body of literature supporting bladder preservation.
This finding stands in contrast to that of Kozak et al, whose analysis of an earlier era found that RT utilization remained unchanged [13]. There are several plausible explanations for increased utilization rates of RT for MIBC. Over the time period studied, there may have been increasing awareness, both among patients and physicians, of bladder preservation therapy as a feasible alternative to cystectomy. Also possible is that as physicians whose training incorporated increased utilization of bladder preservation therapy entered clinical practice, the appeal of this treatment approach increased. Additionally, it is possible that the continued improvements in other fields of medicine better enabled management of comorbid conditions and subsequently increased the number of patients who were eligible for bladder preservation with RT. Due to the limitations of data available in the SEER, our study cannot definitively provide insight into this trend, which is likely to be multifactorial.
The second aim of our study was to evaluate survival outcomes over time for patients receiving RT, and we found that both CSS and OS were improved for patients diagnosed after 2010 as compared with earlier years. This finding is consistent with the largest published institutional experience of bladder preservation therapy to date, which showed that 5-year disease-specific survival improved from 60% in 1986–1995 to 84% in 2005–2013 [15]. Those outcomes are notably better than our reported rates of CSS, but may reflect a more selective group of patients treated at a single institution with demonstrated expertise in bladder preserving therapy. In contrast, our SEER results are representative of a more geographically diverse patient population and clinical practice types.
One likely explanation for the observed improvements in survival outcomes is wider incorporation of RT delivered with concurrent chemotherapy as evidence emerged supporting the superiority of this approach as compared with RT alone. In 2012, a randomized trial by James et al. showed a 32% benefit in disease-free survival with the addition of concurrent flurouracil and mitomycin C to RT, without a significant increase in treatment-related adverse events [8]. Based on these results and other studies [16-19], patients treated more recently were probably more likely to receive concurrent chemotherapy with RT, but unfortunately this information is not available in SEER. Additionally, there have also been improvements in RT technique, such as image-guided treatment and intensity-modulated RT, which over time have become more widely adopted. These technological advantages can allow more accurate targeting of bladder tumors and delivery of higher doses of more conformal radiation, which could further improve treatment efficacy. Recent clinical improvements could also be related to increased use of maximal safe transurethral resection, stage migration, and improved patient selection due to improved and increasingly utilized diagnostic imaging.
Figure 1. Percent utilization of RT compared with cystectomy over time. Gray, cystectomy; black, radiotherapy.
Figure 2. Median patient age by treatment group over the study period. Squares, cystectomy; triangles, radiotherapy.
Table 3. Multivariable Cox model of cancer-specific mortality for patients receiving RT for bladder cancer.
| Variable | HR (95% CI) | P value | |
|---|---|---|---|
| Age (years) | |||
| 21–49 | 1.00 (ref) | ||
| 50–59 | 1.31 (0.86–1.98) | 0.207 | |
| 60–69 | 1.33 (0.89–1.98) | 0.163 | |
| 70–79 | 1.75 (1.19–2.59) | 0.005 | |
| 80–89 | 2.23 (1.51–3.30) | < 0.001 | |
| ≥ 90 | 2.82 (1.86–4.29) | < 0.001 | |
| Sex | |||
| Female | 1.00 (ref) | ||
| Male | 0.86 (0.78–0.95) | 0.004 | |
| Race | |||
| White | 1.00 (ref) | ||
| Hispanic | 1.10 (0.89–1.35) | 0.390 | |
| Black | 1.31 (1.13–1.53) | < 0.001 | |
| Asian | 0.99 (0.79–1.24) | 0.913 | |
| Other or unknown | 0.82 (0.37–1.83) | 0.627 | |
| Marital status | |||
| Married | 1.00 (ref) | ||
| Single | 1.18 (1.01–1.38) | 0.041 | |
| Separated | 1.35 (0.82–2.22) | 0.241 | |
| Divorced | 1.35 (1.13–1.61) | < 0.001 | |
| Widowed | 0.95 (0.85–1.07) | 0.423 | |
| Unmarried | 1.34 (0.19–9.57) | 0.774 | |
| Unknown | 1.16 (0.91–1.49) | 0.237 | |
| Tumor differentiation | |||
| Well | 1.00 (ref) | ||
| Moderately | 1.19 (0.70–2.02) | 0.517 | |
| Poorly | 1.19 (0.72–1.97) | 0.489 | |
| Undifferentiated | 1.15 (0.70–2.02) | 0.576 | |
| Unknown | 1.41 (0.83–2.39) | 0.206 | |
| Histology | |||
| Urothelial carcinoma | 1.00 (ref) | ||
| Adenocarcinoma | 0.76 (0.48–1.19) | 0.231 | |
| Squamous cell carcinoma | 1.34 (1.08–1.66) | 0.008 | |
| Year of diagnosis | |||
| 1992 to 1996 | 1.00 (ref) | ||
| 1997 to 2001 | 1.09 (0.92–1.29) | 0.348 | |
| 2002 to 2005 | 1.02 (0.87–1.21) | 0.809 | |
| 2006 to 2009 | 1.03 (0.87–1.23) | 0.699 | |
| 2010 to 2013 | 0.81 (0.67–0.97) | 0.021 | |
| Stage | |||
| T2 | 1.00 (ref) | ||
| T3 | 1.13 (1.01–1.28) | 0.036 | |
| T4 | 1.57 (1.31–1.88) | < 0.001 | |
On multivariable analysis, we did find race, marital status, and histology to be statistically significantly associated with ACM and CSM. Black race was associated with worse oncologic outcomes. This finding is aligned with prior SEER analyses and may be related to socioeconomic factors, accessibility of care, and potential differences in tumor biology [20]. Outcomes were improved in married patients, which is also likely multifactorial [21]. In our data, squamous cell histology was associated with adverse outcomes, which is also aligned with previous studies [22]. After adjusting for these factors, we did find that compared with patients diagnosed 1992 to 1996, those diagnosed 2010 to 2013 showed improved ACM and CSM. For all other years evaluated, the differences were not statistically significant, suggesting that recent outcomes for patients receiving bladder preservation therapy might be improved.
Unfortunately, there is no randomized data comparing bladder preservation therapy with cystectomy. One attempted study, the Selective Bladder Preservation Against Radical Excision (SPARE) trial, was terminated after failing to accrue: the majority of patients refusing randomization at the time of consent expressed a preference for bladder preservation therapy [23]. Although non-randomized comparisons between RT and surgery are inherently biased to favor surgery, systematic literature review and meta-analysis does not support the notion that better outcomes result from a particular approach [24-26]. We did not attempt to use SEER to compare survival outcomes between patients receiving RT and cystectomy, because the SEER Program will no longer include the “receipt of radiation” variable without signed recognition from the investigator of the “potential biases associated with radiation data”—an explicit acknowledgement of bias [27].
Limitations of this study are primarily related to the absence of complete patient characteristics data and clinical details that are not included in SEER. As such, our analysis was unable to incorporate patient comorbidities, performance status, dose of RT delivered (e.g., curative versus palliative), and information regarding chemotherapy. Another limitation is that in comparing staging between treatment groups, patients who received RT were clinically staged, whereas cystectomy patients were surgically staged. Additionally, for the purposes of reporting CSS, patients were excluded who had a history of non-bladder malignancy prior to our evaluation of utilization rates of RT. However, patients with multiple malignancies would seem less likely to be considered favorable surgical candidates so that exclusion likely does not detract from our conclusion of there being increased utilization of RT relative to cystectomy over time.
In conclusion, our analysis of a large set of cancer registries in the United States provides an update on the use of RT for localized MIBC across the United States and demonstrates that utilization has increased over time relative to cystectomy. Although this increase was modest, it stands in contrast to prior analyses that showed RT utilization rates to be unchanged over time. Moreover, survival outcomes for patients diagnosed after 2010 were improved, perhaps as a result of more uniform adoption of concurrent chemotherapy with RT, as well as higher prevalence of urothelial histology, but also likely at least in part due to better patient selection and improved treatment technique. These findings are notable and support continued efforts to improve and employ bladder preservation strategies utilizing RT for patients with localized MIBC who favor an organ-sparing curative treatment approach.
Figure 3. Three-year OS (A) and CSS (B) of patients receiving RT for bladder cancer stratified by year of diagnosis.
Acknowledgments
None.
References
American Cancer Society (2017) Cancer Facts & Figures 2017. Atlanta: American Cancer Society. Available from: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2017.html [Google Scholar]
Kaufman DS, Shipley WU, Feldman AS (2009) Bladder cancer. Lancet 374: 239-249. doi: 10.1016/S0140-6736(09)60491-8. [View Article] [PubMed] [Google Scholar]
Grossman HB, Natale RB, Tangen CM, Speights VO, Vogelzang NJ, et al. (2003) Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 349: 859-866. doi: 10.1056/NEJMoa022148. [View Article] [PubMed] [Google Scholar]
Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, et al. (2001) Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol 19: 666-675. doi: 10.1200/JCO.2001.19.3.666. [View Article] [PubMed] [Google Scholar]
Zehnder P, Studer UE, Skinner EC, Dorin RP, Cai J, et al. (2011) Super extended versus extended pelvic lymph node dissection in patients undergoing radical cystectomy for bladder cancer: a comparative study. J Urol 186: 1261-1268. doi: 10.1016/j.juro.2011.06.004. [View Article] [PubMed] [Google Scholar]
Shabsigh A, Korets R, Vora KC, Brooks CM, Cronin AM, et al. (2008) Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. Eur Urol 55: 164-174. doi: 10.1016/j.eururo.2008.07.031. [View Article] [PubMed] [Google Scholar]
Rödel C, Grabenbauer GG, Kühn R, Papadopoulos T, Dunst J, et al. (2002) Combined-modality treatment and selective organ preservation in invasive bladder cancer: long-term results. J Clin Oncol 20: 3061-3071. doi: 10.1200/JCO.2002.11.027. [View Article] [PubMed] [Google Scholar]
James ND, Hussain SA, Hall E, Jenkins P, Tremlett J, et al. (2012) Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med 366: 1477-1488. doi: 10.1056/NEJMoa1106106. [View Article] [PubMed] [Google Scholar]
Kaufman DS, Shipley WU, Griffin PP, Heney NM, Althausen AF, et al. (1993) Selective bladder preservation by combination treatment of invasive bladder cancer. N Engl J Med 329: 1377-1382. doi: 10.1056/NEJM199311043291903. [View Article] [PubMed] [Google Scholar]
Hagan MP, Winter KA, Kaufman DS, Wajsman Z, Zietman AL, et al. (2003) RTOG 97-06: initial report of a phase I-II trial of selective bladder conservation using TURBT, twice-daily accelerated irradiation sensitized with cisplatin, and adjuvant MCV combination chemotherapy. Int J Radiat Oncol Biol Phys 57: 665-672. doi: 10.1016/S0360-3016(03)00718-1. [View Article] [PubMed] [Google Scholar]
Kaufman DS, Winter KA, Shipley WU, Heney NM, Wallace 3rd, et al. (2008) Phase I-II RTOG study (99-06) of patients with muscle-invasive bladder cancer undergoing transurethral surgery, paclitaxel, cisplatin, and twice-daily radiotherapy followed by selective bladder preservation or radical cystectomy and adjuvant chemotherapy. Urology 73: 833-837. doi: 10.1016/j.urology.2008.09.036. [View Article] [PubMed] [Google Scholar]
Mak RH, Hunt D, Shipley WU, Efstathiou JA, Tester WJ, et al. (2014) Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: a pooled analysis of Radiation Therapy Oncology Group protocols 8802, 8903, 9506, 9706, 9906, and 0233. J Clin Oncol 32: 3801-3809. doi: 10.1200/JCO.2014.57.5548. [View Article] [PubMed] [Google Scholar]
Kozak KR, Hamidi M, Manning M, Moody JS (2012) Bladder preservation for localized, muscle-invasive bladder cancer: the survival impact of local utilization rates of definitive radiotherapy. Int J Radiat Oncol Biol Phys 83: 197-204. doi: 10.1016/j.ijrobp.2011.12.038. [View Article] [PubMed] [Google Scholar]
Giacalone NJ, Shipley WU, Clayman RH, Niemierko A, Drumm M, et al. (2017) Long-term Outcomes After Bladder-preserving Tri-modality Therapy for Patients with Muscle-invasive Bladder Cancer: An Updated Analysis of the Massachusetts General Hospital Experience. Eur Urol 71: 952-960. doi: 10.1016/j.eururo.2016.12.020. [View Article] [PubMed] [Google Scholar]
Efstathiou JA, Spiegel DY, Shipley WU, Heney NM, Kaufman DS, et al. (2011) Long-term outcomes of selective bladder preservation by combined-modality therapy for invasive bladder cancer: the MGH experience. Eur Urol 61: 705-711. doi: 10.1016/j.eururo.2011.11.010. [View Article] [PubMed] [Google Scholar]
Mitin T, Hunt D, Shipley WU, Kaufman DS, Uzzo R, et al. (2013) Transurethral surgery and twice-daily radiation plus paclitaxel-cisplatin or fluorouracil-cisplatin with selective bladder preservation and adjuvant chemotherapy for patients with muscle invasive bladder cancer (RTOG 0233): a randomised multicentre phase 2 trial. Lancet Oncol 14: 863-872. doi: 10.1016/S1470-2045(13)70255-9. [View Article] [PubMed] [Google Scholar]
Zapatero A, Martin De Vidales, Arellano R, Ibañez Y, Bocardo G, et al. (2012) Long-term results of two prospective bladder-sparing trimodality approaches for invasive bladder cancer: neoadjuvant chemotherapy and concurrent radio-chemotherapy. Urology 80: 1056-1062. doi: 10.1016/j.urology.2012.07.045. [View Article] [PubMed] [Google Scholar]
Lagrange J, Bascoul-Mollevi C, Geoffrois L, Beckendorf V, Ferrero J, et al. (2010) Quality of life assessment after concurrent chemoradiation for invasive bladder cancer: results of a multicenter prospective study (GETUG 97-015). Int J Radiat Oncol Biol Phys 79: 172-178. doi: 10.1016/j.ijrobp.2009.10.038. [View Article] [PubMed] [Google Scholar]
Aizer AA, Wilhite TJ, Chen M, Graham PL, Choueiri TK, et al. (2014) Lack of reduction in racial disparities in cancer-specific mortality over a 20-year period. Cancer 120: 1532-1539. doi: 10.1002/cncr.28617. [View Article] [PubMed] [Google Scholar]
Aizer AA, Chen M, McCarthy EP, Mendu ML, Koo S, et al. (2013) Marital status and survival in patients with cancer. J Clin Oncol 31: 3869-3876. doi: 10.1200/JCO.2013.49.6489. [View Article] [PubMed] [Google Scholar]
Scosyrev E, Yao J, Messing E (2009) Urothelial carcinoma versus squamous cell carcinoma of bladder: is survival different with stage adjustment?. Urology 73: 822-827. doi: 10.1016/j.urology.2008.11.042. [View Article] [PubMed] [Google Scholar]
Huddart RA, Hall E, Lewis R, Birtle A (2010) Life and death of spare (selective bladder preservation against radical excision): reflections on why the spare trial closed. BJU Int 106: 753-755. doi: 10.1111/j.1464-410X.2010.09537.x. [View Article] [PubMed] [Google Scholar]
Gray PJ, Lin CC, Jemal A, Shipley WU, Fedewa SA, et al. (2014) Clinical-pathologic stage discrepancy in bladder cancer patients treated with radical cystectomy: results from the national cancer data base. Int J Radiat Oncol Biol Phys 88: 1048-1056. doi: 10.1016/j.ijrobp.2014.01.001. [View Article] [PubMed] [Google Scholar]
Kulkarni GS, Hermanns T, Wei Y, Bhindi B, Satkunasivam R, et al. (2017) Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in the setting of a multidisciplinary bladder cancer clinic. J Clin Oncol 35: 2299-2305. doi: 10.1200/JCO.2016.69.2327. [View Article] [PubMed] [Google Scholar]
Vashistha V, Wang H, Mazzone A, Liss MA, Svatek RS, et al. (2016) Radical cystectomy compared to combined modality treatment for muscle-invasive bladder cancer: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys 97: 1002-1020. doi: 10.1016/j.ijrobp.2016.11.056. [View Article] [PubMed] [Google Scholar]
National Cancer Institute (2017) Surveillance, Epidemiology, and End Results Program. Radiation/Chemotherapy Databases. Available from: https://seer.cancer.gov/data/treatment.html [Google Scholar]